Atrial Fibrillation
- Arrhythmia Databases
- Physionet
- Physionet Database
General1¶
- Most Common sustained Arrhythmia
- 95% of patients are > 60 y/o
- Causes: Atrial enlargement, elevated atrial pressure, atrial infiltration or inflammation
- Leads to increase in LA load and thus LA pressure thus predisposes to afib
- Precipitants of atrial dilation and/or conduction remodeling
- Advanced age
- Systemic hypertension (MC underlying condition)
- MV dysfunction (MS/MR)
- LV failure (CHF)
- CAD and related factors (T2DM and smoking)
- Obesity and OSA
- Chronic hypoxic lung disease (COPD)
- Alcohol
- Triggers of increased automaticity
- Subclinical or Overt Hyperthyroidism
- Excessive alcohol use
- Increased sympathetic tone
- Acute illness (sepsis, PE, MI, myocarditis)
- Cardiac Surgery (Post cardiac surgery due to pericarditis)
- Sympathomimetic drugs (cocaine, theophylline, amphetamines)
Definitions¶
Paroxysmal AFib (≥2 episodes that terminate spontaneously or with intervention within 7 days of onset)¶
- 70% at one year to 90% at 4 years of recurrence
- Triggers: Ectopic Foci (Pulmonary Ventricular sites)
- Treatment:
- Amiodarone, Flecainide, sometimes Ablation (works better): Pulmonary vein potentials in the LA
Persistent AFib (≥2 episodes, each lasts >7 days)¶
- Triggers: Electrophysiologic remodeling fibrosis
- SVC or coronary sinus most commonly
- Non-Pulmonary Ventricle sites
- Treatment
- Cardioversion if unstable
- Medical therapy
- Ablation usually doesn’t work, try after medicine
Long-standing Persistent or Permanent AFib (>6-12 months)¶
- Triggers: Chronic Substrate Fibrosis
AFib w/ Rapid Ventricular Response (RVR)¶
- HOCM, HFpEF, Impaired cardiac function
- Symptoms
- Exercise intolerance, fatigue, palpitations, chest pain, light headedness, hemodynamic instability
- Tachycardia-mediated cardiomyopathy
Features¶
- Irregularly irregular rhythm w/ Narrow QRS and variable p waves
- No distinct P waves, absent A waves, narrow QRS
- Rate: 100-110 BPM
- Disorganized atrial impulses all over the atria
- Usually starts in LA (Pulmonary veins)
- MC location of ectopic foci (ablate them)
- Multiple reentrant circuits that coexist
- P waves occur at a rate between 350-600, ventricular rates slower than atrial rates
- Rate is determined by AV nodal conduction; arises from uncoordinated or loss of atrial contraction (Chaotic rapid atrial electrical activity)
- No distinct P waves, absent A waves, narrow QRS
- Tachycardia may continue despite beats that fail to conduct to the ventricles, indicating that the AV node is not participating in the tachycardia circuit
- Ashman Phenomenon: Aberrantly conducted beats after long-short R-R cycles
Complications¶
- Loss of atrial contributions to ventricular filling
- Predisposition to thrombus formation in the left atrial appendage w/potential embolization (Thromboembolic Stroke)
- In patients with MS or HOCM, conversion to sinus rhythm increases embolic risk
- More likely for stoke 5x
Diagnosis and Work-up¶
- Diagnosis: EKG to Confirm
- TTE and TSH/Free T4
- To assess for atrial thrombi, hyperthyroidism, baseline for long-term
- Hypertension MCC
- TEE if TTE shows valvular disease
- Exercise stress test after starting medications
- Holter, telemetry to identify asymptomatic episodes
- EPS: to test for SVTs (AVNRT/MAT)
- TTE and TSH/Free T4
- W/U: CMP, TSH, Echo
Management2¶
Rhythm/Rate¶
- AFFIRM3: Rate-control = Rhythm-control; Rate preferred due to Adverse events
- Rate vs Rhythm Control in Recurrent Persistent Afib
- Early Rhythm Control
- Goal: HR<80 if symptoms, HR <110 if none, EF >40%
- EAST-AFNET 4*
- Improved clinical outcomes if early rhythm control in all patients diagnosed within the past 12 months w/coexisting CVD
- Aggressive rhythm control via Ablation or Amiodarone
- EAST-AFNET 4*
- Goal: HR<80 if symptoms, HR <110 if none, EF >40%
- RACE-II: Lenient non-inferior to strict rate-control in afib
- RAAFT-2: RFA if AAD failed as 1st line for symptomatic PAF
- RFA recommended in patients with symptomatic PAF who have failed treatment with at least 1 Class I or Class III AAD
Acute Afib w/RVR¶
Unstable Afib w/RVR¶
- Immediate Cardioversion
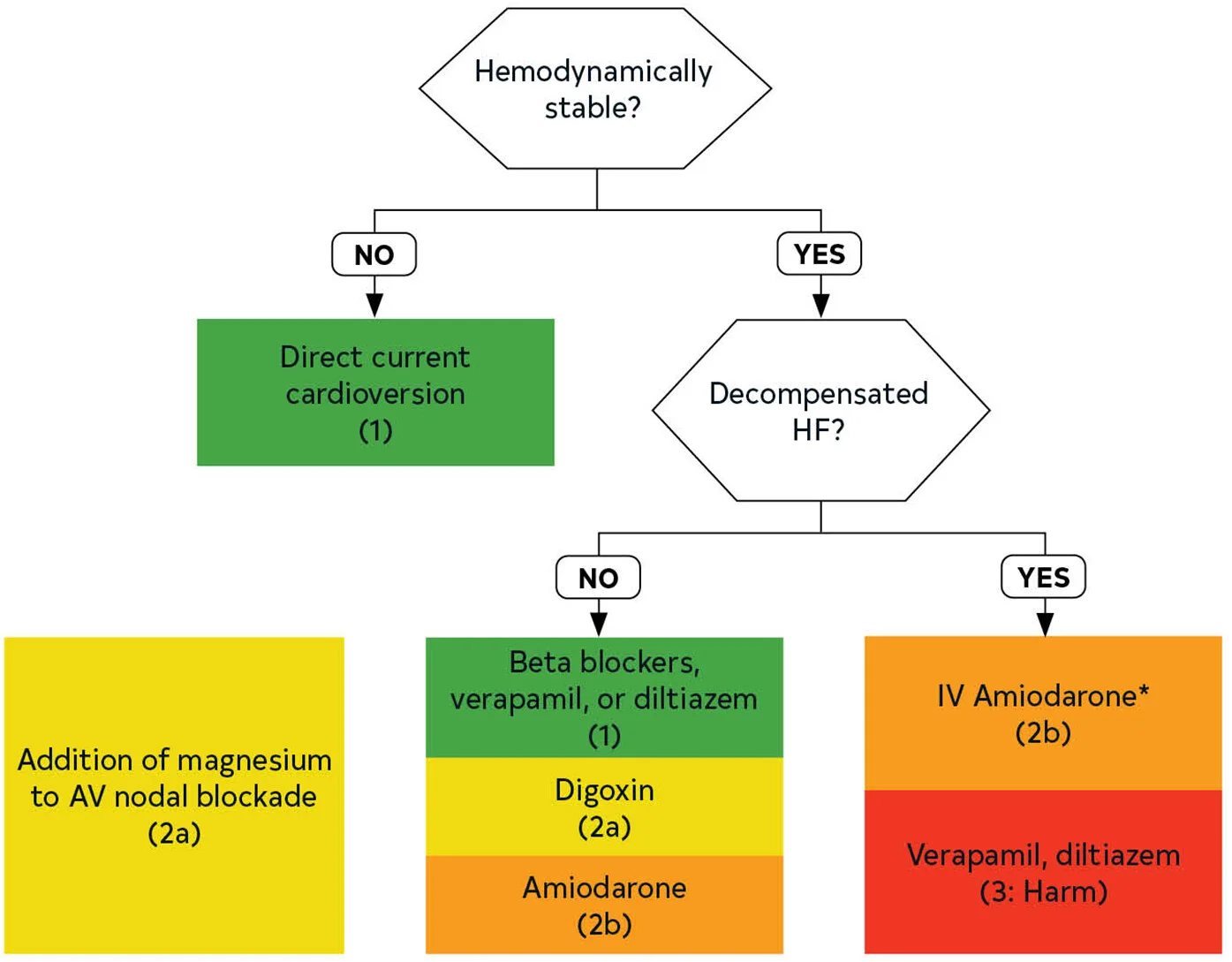
Stable Afib w/RVR¶
-
1B: Non-dihydropyridine CCBs or BBs
- Severe COPD: CCBs (Cardizem)
- CAD: BBs (Metoprolol Tartrate)
-
2A: IV Magnesium
- 2A: Digoxin if can't use BBs or CCBs
- Total IV loading dose:
- Normal renal function: 8-12 mcg/kg ideal body weight (usually ~600-1,000 mcg).
- Renal insufficiency: 6-10 mcg/kg ideal body weight.
- Typically, 50% of the total loading dose is given initially, followed by 25% given twice, every six hours.
- The first IV dose (typically ~400-600 mcg) takes effect within roughly 1-4 hours. Monitor for effect. If an adequate heart rate is achieved, then subsequent doses may be omitted. If bradycardia occurs, further administration should be held
- Total IV loading dose:
- 2B: Amiodarone
- Radiofrequency Ablation (RFA)
- 1 year success rates approach 70-80%
- Afib recurrence after RFA in 20-40% of patients
- OSA independently increases the risk of incident atrial fibrillation and increases the risk of recurrent AF after ablation by promoting atrial structural and electrical remodeling including atrial enlargement and low-voltage areas with conduction abnormalities
- Treatment of OSA with CPAP improves arrhythmia-free survival post-catheter ablation
- Repeat ablation is primarily considered for those with symptomatic AF recurrences (often drug-refractory) occurring at least 3 months or more post-ablation
- At 1-year follow-up more patients randomized to repeat ablation with RF (58%) were AF-free compared with those who underwent cryoablation (43%)5
- OSA independently increases the risk of incident atrial fibrillation and increases the risk of recurrent AF after ablation by promoting atrial structural and electrical remodeling including atrial enlargement and low-voltage areas with conduction abnormalities
- Complications (<5%)
- Stroke
- Pulmonary Vein Stenosis
- Esophageal injury
- Phrenic Nerve Paralysis
- Acute Pericarditis (10.2%)
Anticoagulation¶
- Trials
- Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report
- AVERROES: Eliquis > Aspirin alone for Stroke/VTE
- ARISTOTLE: Eliquis > Warfarin for stroke, less brain bleeding
- ROCKET-AF: Xarelto is non-inferior to Warfarin
- BRIDGE: Periprocedural bridging did not reduce ATE, increased bleeding
- Non-Valvular Afib
- CHA2DS2-VASc Score (stroke risk, max is 9)
- Anticoagulation in Non-valvular Atrial Fibrillation
- CHF, Hypertension, DM, Vascular disease (prior MI, PAD, or aortic plaque), age 65-74, female (all 1)
- Age ≥75, Stroke/TIA/Thromboembolism (all 2)
- 0 (Low Risk): None
- 1 in males (Moderate) or 2 in females: None or aspirin or oral anticoagulants
- ≥2 in males (high) or ≥3 in females: Oral Anticoagulants
- Use warfarin at INR 2-3 or non-vitamin K antagonist oral anticoagulants to prevent thromboembolism
- Risk
- 0: 0.2% annual stroke risk
- 1: 0.6%
- 2: 2.2%
- 3: 3.2%
- 4: 4.8%
- 5: 7.2%
- 6: 9.7%
- 7: 11.2%
- 8: 10.8%
- 9: 12.2%
- Treatment
- Positive net clinical benefit of chronic AC in patients with high thromboembolic risk
- DOACs Preferred
- Similar or reduced risk of stroke, reduced risk of major bleeding and hemorrhagic stroke in patients with CKD and eGFR ≥304
- DOACs > Warfarin in CKD for Nonvalvular Afib
- Dabigatran vs. Warfarin
- CHA2DS2-VASc Score (stroke risk, max is 9)
- Valvular Afib
- Severe Mitral Stenosis (Valve area ≤1.5cm^2)
- Mechanical Heart Valve (any location)
- RF: Afib, LV systolic dysfunction, prior VTE, hypercoagulable state
- INR target 1.5 may be reasonable in newer valves
- Risk of VTE is 4% per year without AC, 2% with aspirin, <1% with warfarin
- Modern Bileaflet Aortic Valve w/o RF: INR 2.0-3.0
- Mitral Valve: INR 2.5-3.5
- Aortic Valve w/≥1 RF: INR 2.5-3.5
- Aortic Valve with old-generation valve: INR 2.5-3.5
- Low-dose Aspirin: only in patients with other strong indications (Severe CAD)
- Dabigatran vs. Warfarin
- RF: Afib, LV systolic dysfunction, prior VTE, hypercoagulable state
- Treatment