Ventricular Arrhythmias
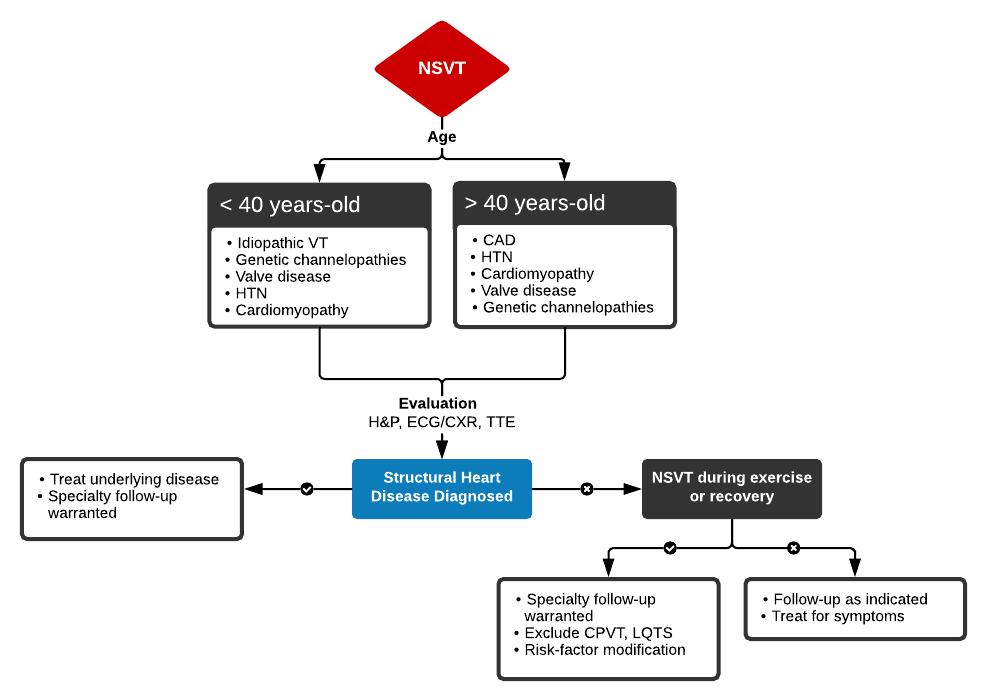
Nonsustained Ventricular Tachycardia (NSVT)¶
- ≥3-5 consecutive ventricular beats lasting <30s
- Patient remains hemodynamically stable
- 0-4% of ambulatory patients
- Frequently asymptomatic
- W/U: EKG ± CXR/TTE
- Treatment
- Admit if
- High-Risk (Age >45, Symptomatic, Known SHD, Concerning FH)
- Admit if
General¶
- Patients with CHD and LV systolic dysfunction are at increased risk of ventricular arrythmias including VT and VF
- 95% of wide complex tachycardias are VT in pts with SHD
- Associated with
- Dilated Cardiomyopathies, Brugada’s syndrome, HCM, Amyloidosis/Sarcoidosis, Duchenne Muscular Dystrophy, TOF, and myocarditis
- Treatment in patients with Recurrent VT
- 1) Stabilize
- 2) Find underlying cause (electrolyte abnormalities)
- Order Electrolyte panel and Digoxin level
- Hypokalemia and hypomagnesemia (loop diuretics)
- Digoxin ± Hypokalemia
Types¶
1) Fast Ventricular Tachycardias - Monomorphic VT (MVT) - Sustained Monomorphic VT (SMVT) - Polymorphic VT (PVT) 2) Slow Ventricular Tachycardias 3) Ventricular Fibrillation
Fast Ventricular Tachycardias¶
-
3 consecutive premature ventricular beats (widened QRS)
- Wide QRS complex tachycardia often w/ abnormal QRS complexes and T waves in the vector opposite of the QRS
- Common, along with Vfib, post MI
- Pulse or pulseless presentation
Monomorphic Ventricular Tachycardia (MVT)¶
- Etiology
- Rapid and repetitive firing of ≥3 premature ventricular complexes in a row with the same morphology
- Macro re-entrant circuit with conduction through and around scar tissue, reentry of an ectopic ventricular depolarization
- May be post MI (reentry)
- QRS wide (>0.12), uniform and stable, rate between 100-250
- AV dissociation may be apparent (regular rate between p waves)
- Cannon A waves in the neck
- Capture beats and fusion beats possible
- Symptoms
- Palpitations, dyspnea, lightheadedness, angina, or near-syncope, syncope, seizures
- Treatment
- Stable/Pulse: IV amiodarone, metoprolol, revascularization OR Synchronized cardioversion
- Pulseless: CPR + Defibrillation ± Vasopressors
Sustained Monomorphic Ventricular Tachycardia (SMVT)¶
- Wide complex tachycardia with 2 fusion beats
- Fusion beats: capture of electrical signal though both the atrium and ventricle briefly
- Hybrid of a normal and wide QRS complex (P waves precede fusion complex)
- Treatment
- Stable: IV Amiodarone > Procainamide, sotalol, lidocaine
- Unstable: Synchronized Cardioversion
Polymorphic Ventricular Tachycardia (PVT)¶
- Triggered tachycardia, >220 can cause Ventricular Fibrillation
- Wide complex, rapid and unstable
- QRSs vary in amplitude, size, and duration
- Normal QTc = Coronary Ischemia (MI)
- Prolonged QTc = Torsade De Pointes
- Men >440ms, women >460ms
- A) Torsade De Points (Polymorphic VT, TdP)
- A rapid PVT with PVCs before T wave, may cause syncope
- VT with constantly changing cycle length, axis, and morphology
- Onset: prolongation/lengthening of the QT interval which can be initiated by a PAC/PVC
- Causes: Hypokalemia, hypomagnesemia, genetic Long QT
- Medications increasing QT interval via inhibition of the rapid components of the delayed rectifier potassium current (Ikr)
- Meds: Chloroquine, hydroxychloroquine, azithromycin
- RF for drug induced: QTc >500ms, QTc lengthening >60ms, female, age >65, bradycardia, hypokalemia, hypomagnesemia, hypocalcemia, HFrEF, ≥2 QT prolonging drugs, rapid IV admin
- 30% have mutation in one of 5 QT syndrome genes
- Goals
- K >4, Mg >2, EKG q3-6m
- Baseline then annually if on methadone, daily if >120mg
- Treatment
- Stable
- IV Magnesium sulfate, avoid QT prolongation, lidocaine, increase HR (shortens QT)
- Even if normal serum Mg
- Temporary pacemaker, isoproterenol
- IV Magnesium sulfate, avoid QT prolongation, lidocaine, increase HR (shortens QT)
- Unstable: Defibrillation
- Stable
General Management¶
- Pulse + Stable and Sustained Monomorphic
- IV Amiodarone > lidocaine
- CI: Hypotension/unstable
- Immediate Cardioversion if amiodarone fails
- IV Amiodarone > lidocaine
- Pulse + Unstable and Sustained Monomorphic
- Synchronized Cardioversion
- Low energy shock to QRS complex that is timed
- IV amiodarone to prevent VT/VF after Cardioversion
- Synchronized Cardioversion
- Pulseless
- 1) Defibrillation (unsynchronized Cardioversion)
- High energy shock at a random point, multiple attempts
- 2) Epinephrine every 3-5 mins
- 3) Amiodarone/Lidocaine
- 1) Defibrillation (unsynchronized Cardioversion)
- Chronic: ICD
Slow Ventricular Tachycardias(40-150 BPM)¶
Ventricular escape (3rd degree AV Block)¶
Accelerated Ventricular Rhythm¶
Idioventricular¶
Ventricular Fibrillation (VF)¶
- Chaotic, irregular waveform of varying shapes and amplitude
- No coordinated contractions, identifiable p waves, QRS, or T waves
- Very rapid, irregular polymorphic rhythm
- Disorganized electrical activity with multiple rapidly firing foci in the ventricles (Ventricles can’t produce CO)
- Diffuse wide QRS segments
- Pulseless tachyarrhythmia
- Most begin with Vtach
- RF: IHD, antiarrhythmics, Atrial fib w/RVR
- Common in patients with MI
- Most common cause of SCD during acute MI
- Treatment
- Immediate Defibrillation + CPR
- IV Epinephrine or Vasopressin without interrupting CPR if 1st defibrillation doesn’t work
- IV amiodarone
- Immediate Defibrillation + CPR